
For millions of men, stubborn chest fat — often called “man boobs” — is a source of profound frustration and quiet insecurity. The standard fitness script is predictable: do more bench presses, grind through cable flyes, slash your calories, and log endless hours on the treadmill.
Yet after months of disciplined execution, many men look in the mirror and see the exact same soft, puffy chest staring back at them. Their shirts still fit awkwardly. Their confidence stays buried. And they are left asking one question: What am I doing wrong?
The answer is both frustrating and liberating: stubborn chest fat is rarely a chest problem — it is a systemic hormonal problem.
When you attack a biochemical imbalance using purely mechanical tools like chest isolation exercises, you are fighting the wrong battle entirely. To permanently flatten your chest and reclaim a masculine physique, you must understand the biological switches that govern male fat distribution — and learn how to flip them.
This comprehensive guide breaks down the precise science behind how to get rid of chest fat. It covers the hormonal mechanisms driving fat storage, the nutritional strategies that restore insulin sensitivity, and the exercise and lifestyle protocols that permanently interrupt the cycle — backed by peer-reviewed research and updated with the most current data available in 2026.
1. Pseudo-Gynecomastia vs. True Gynecomastia: Know Your Enemy
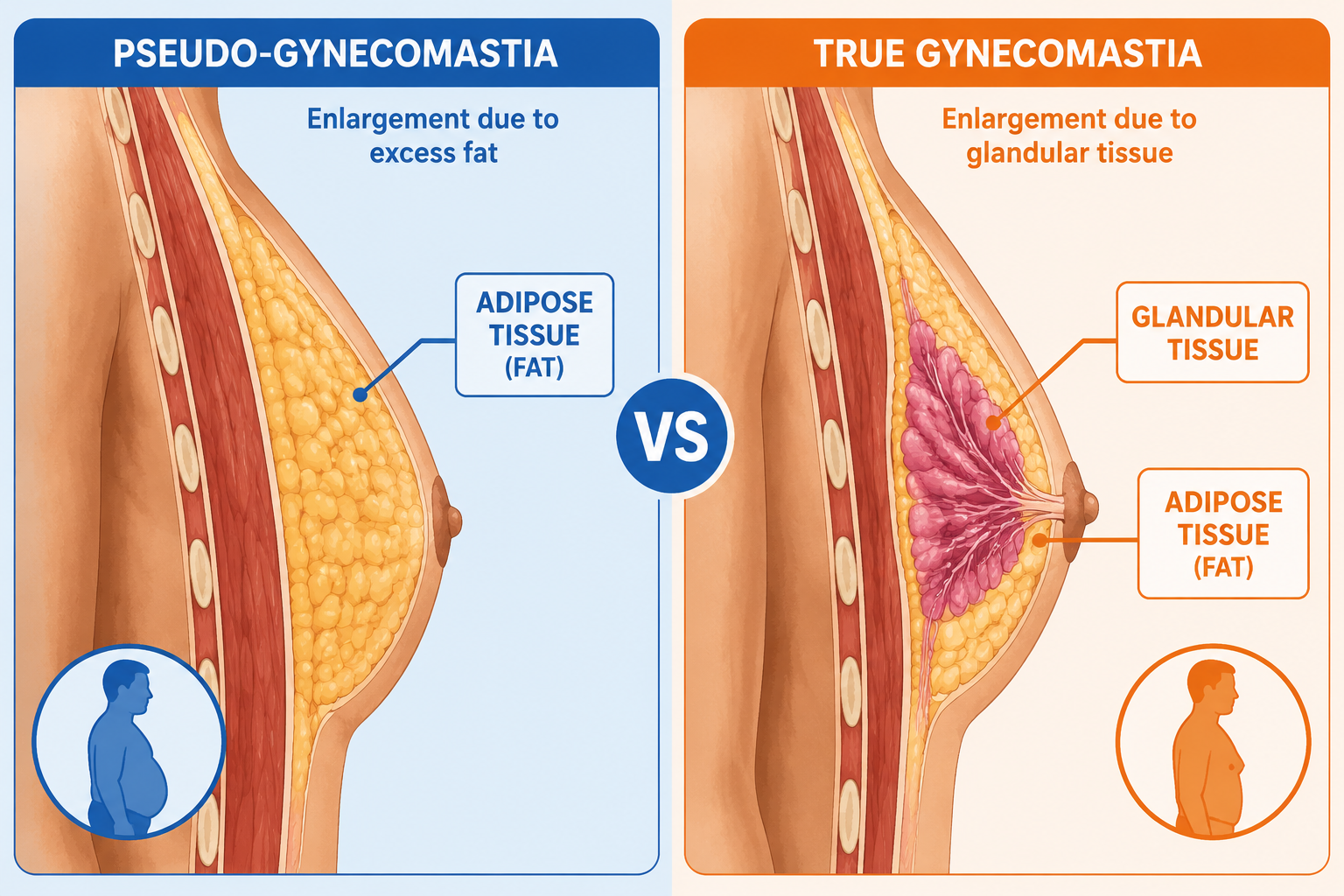
![Split medical diagram showing pseudo-gynecomastia vs true gynecomastia cross-section, clean infographic style, labeled adipose tissue and glandular tissue, blue and orange color scheme]
Before deploying any strategy, you need to understand exactly what type of tissue you are dealing with. Chest fat in men manifests in two distinct forms, and each one requires a fundamentally different understanding of biology.
Pseudo-Gynecomastia: The Fat-Only Form
Pseudo-gynecomastia is characterized by an accumulation of excess subcutaneous adipose tissue — plain fat — across the pectoral region. There is no underlying structural abnormality or significant hormonal pathology at play. It is simply the byproduct of carrying a high overall body fat percentage.
Key characteristics include:
- Soft, uniform texture across the entire chest without a distinct lump behind the nipple
- No tenderness or sensitivity when the chest is pressed
- Proportional reduction when overall body fat drops through a sustained caloric deficit
- Symmetrical appearance on both sides of the chest
If you have pseudo-gynecomastia, the path forward is clearer — though not necessarily easy. As your total body fat percentage descends, your chest will shrink along with it. The hormonal optimization strategies in this guide will dramatically accelerate that process.
True Hormonal Gynecomastia: The Glandular Form
True gynecomastia is a different beast entirely. It is driven by a profound disruption in the systemic ratio of circulating testosterone to estrogen. While it commonly emerges during puberty, it increasingly affects men over 30 — and by 2026, research from the Journal of Clinical Endocrinology and Metabolism estimates that up to 36% of men over age 40 show measurable signs of clinical gynecomastia, up from 27% a decade ago.
True gynecomastia involves the proliferation of actual glandular breast tissue directly behind the nipple. Distinguishing features include:
- A firm, rubbery disc or lump palpable directly beneath the nipple
- A distinct “puffy nipple” appearance that persists even at lower body fat levels
- Localized tenderness or sensitivity when pressure is applied
- A soft, saggy chest structure that does not respond to diet or exercise the way surrounding body fat does
- Often asymmetrical, with one side more pronounced than the other
Critical note: True gynecomastia that does not respond to lifestyle intervention warrants a visit to an endocrinologist. Certain medications — including anabolic steroids, anti-androgens, some antidepressants, and proton pump inhibitors — are documented causes. A full hormonal blood panel is essential before assuming lifestyle changes alone will resolve the condition.
Understanding which form you are dealing with determines your entire strategy. Most men battling persistent chest fat are caught somewhere on the spectrum between the two — carrying excess subcutaneous fat while simultaneously managing a hormonal environment that makes that fat nearly impossible to shift without targeted intervention.
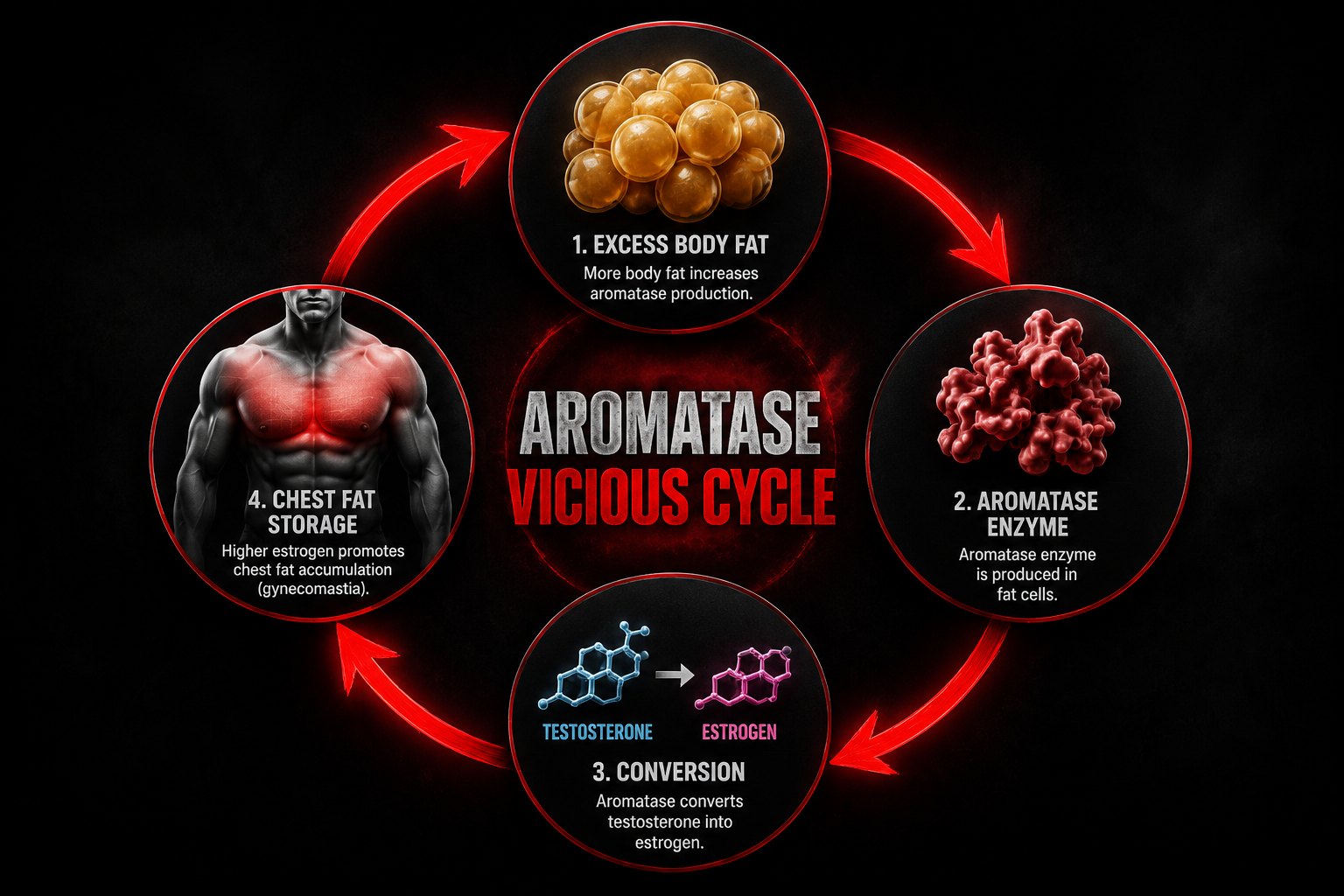
2. The Biochemical Trap: The Aromatase Vicious Cycle
![Circular flowchart infographic showing the Aromatase Vicious Cycle: body fat → aromatase enzyme → testosterone to estrogen conversion → chest fat storage → loop back, dark background with red arrows]
To understand why chest fat is so stubborn, you need to examine how testosterone and estrogen interact inside the male body — and how easily that balance tips in the wrong direction.
In a healthy man in his twenties, testosterone is the dominant androgen. It keeps estrogen tightly regulated, maintains lean muscle mass, and governs where the body prefers to store or burn fat. However, after crossing the threshold of age 30, natural testosterone production begins a steady, unrelenting decline of approximately 1% to 2% per year, as documented in the Journal of Clinical Endocrinology and Metabolism.
A 1% annual decline sounds manageable in isolation. The problem accelerates exponentially because of one enzyme: aromatase.
What Is Aromatase?
Aromatase is the enzyme responsible for the biosynthesis of estrogen in men. It resides predominantly in adipose tissue — specifically the visceral fat surrounding your organs and the subcutaneous fat concentrated on your chest and hips. A landmark study published in the Journal of Steroid Biochemistry and Molecular Biology demonstrated that aromatase activity in fat tissue scales up dramatically as body fat percentage rises.
The result is a self-reinforcing biochemical trap that works like this:
Step 1 — Excess Fat Increases Aromatase Volume
Carrying above-average body fat means you are housing a larger volume of aromatase enzymes throughout your adipose tissue.
Step 2 — Aromatase Converts Testosterone Into Estrogen
These excess enzymes aggressively intercept circulating testosterone molecules and chemically convert them into estradiol — the primary form of estrogen.
Step 3 — Elevated Estrogen Signals Preferential Fat Storage
Rising estrogen levels send a powerful hormonal signal to deposit more fat in estrogen-sensitive areas: the chest, nipples, and hips.
Step 4 — New Chest Fat Generates More Aromatase
The newly deposited chest fat houses additional aromatase enzymes, which further accelerate the testosterone-to-estrogen conversion.
The loop closes — and tightens with every cycle.
Why Traditional Methods Fail Inside This Loop
This is the core reason why chest presses and aggressive cardio fail to solve the problem. A severe caloric deficit or excessive endurance training in this hormonal environment does not preferentially target estrogen-dominant fat zones. Instead, the body — already cortisol-elevated and testosterone-suppressed — preferentially catabolizes lean muscle tissue while stubbornly protecting the chest fat that is being actively maintained by elevated estrogen.
You are not failing because of a lack of effort. You are failing because you are using mechanical tools to solve a biochemical problem.
Breaking the aromatase cycle requires interrupting the chemical signals at their source — which is exactly what the three pillars outlined in this guide are designed to do.
3. The Insulin Connection: The Hormonal Lock on Fat Burning
The second major hormonal driver of stubborn chest fat is chronic insulin elevation, clinically referred to as hyperinsulinemia. Understanding this mechanism is non-negotiable for anyone serious about learning how to get rid of chest fat permanently.
How Insulin Blocks Fat Burning
Insulin is a highly anabolic storage hormone secreted by the pancreas in response to rising blood glucose. When you eat carbohydrates or sugars, blood glucose rises, and insulin is released to ferry that glucose into your cells for energy or storage.
In a metabolically healthy person, this is a clean, efficient process. The problem is modern lifestyle habits — ultra-processed foods, constant snacking, chronic stress, and poor sleep — keep insulin levels chronically elevated throughout the day.
When insulin is elevated, your body is locked into a strict metabolic state of storage. Specifically:
- Lipolysis is completely halted. The enzyme hormone-sensitive lipase (HSL), which breaks down stored fat for fuel, is directly inhibited by insulin. You cannot burn chest fat when insulin is high — full stop.
- Fat synthesis is accelerated. Elevated insulin activates lipoprotein lipase (LPL) in fat cells, actively directing circulating fatty acids into storage.
- Glucose oxidation dominates. Your body burns glucose as its primary fuel source, never reaching the point of tapping into stored body fat.
The Testosterone-Suppressing Effect of High Insulin
The damage extends well beyond simple fat storage. Research published in Diabetes Care revealed that chronically elevated insulin directly suppresses testosterone production by disrupting the hypothalamic-pituitary-gonadal (HPG) axis — the hormonal command chain that signals the testes to produce testosterone.
Simultaneously, hyperinsulinemia amplifies the expression and activity of aromatase within fat cells, directly accelerating the testosterone-to-estrogen conversion described in the previous section.
The compounding effect is devastating:
- High insulin prevents your body from burning existing chest fat
- High insulin lowers your testosterone production
- High insulin amplifies aromatase activity, converting remaining testosterone into estrogen
- Elevated estrogen signals more fat storage on the chest
This is why insulin control is not optional — it is the foundation of every effective chest fat elimination strategy.
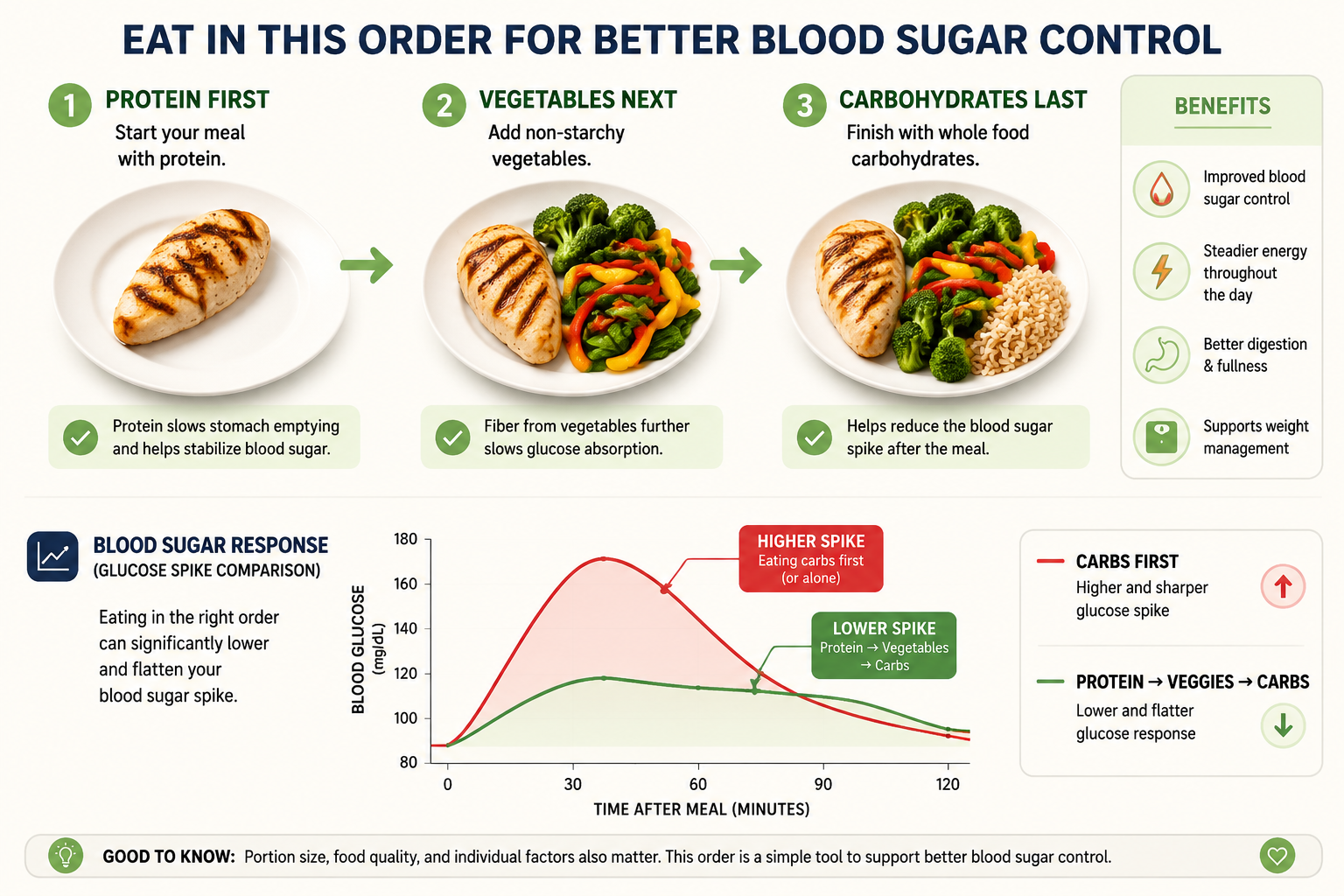
4. Pillar 1: Re-Engineering Your Insulin Response
![Step-by-step food sequencing plate infographic showing protein first, then vegetables, then carbohydrates, with glucose spike comparison graph, clean modern nutrition diagram style]
Fixing your insulin sensitivity does not require starving yourself or eliminating entire food groups. It requires strategic, evidence-based nutrition adjustments that alter the biochemical environment of your digestive tract. Here is exactly how to do it.
Strategy 1: The Food Sequencing Protocol
One of the simplest yet most powerful tools for controlling insulin is changing the order in which you eat the food on your plate. The sequence is non-negotiable:
$$\text{Protein} \longrightarrow \text{Fiber (Vegetables)} \longrightarrow \text{Carbohydrates}$$
A clinical study conducted at Stanford University and published in Diabetes Care tracked participants eating identical meals with identical caloric values but in different sequences. The findings were striking:
- Eating protein and vegetables before carbohydrates reduced post-meal glucose spikes by up to 37%
- The total insulin response was slashed by up to 44%
- These benefits persisted across multiple meal types and were consistent regardless of overall caloric intake
The mechanism is elegant: consuming protein and fiber first coats the digestive tract and slows gastric emptying. When carbohydrates finally reach the small intestine, they are absorbed at a gradual, metered pace rather than flooding the bloodstream all at once. The result is a dramatically blunted insulin response — from the exact same meal.
Practical application:
- Start every meal with 4–6 oz of protein (chicken, eggs, fish, beef)
- Eat your vegetables and salad next
- Only then consume rice, bread, pasta, or other starchy carbohydrates
- This single habit costs nothing and requires no dietary restriction
Strategy 2: The Apple Cider Vinegar Protocol
To further fortify your insulin defense, implement a pre-meal apple cider vinegar (ACV) protocol. The mechanism is grounded in solid biochemistry, not wellness folklore.
The protocol:
Mix 1 tablespoon of raw, unfiltered apple cider vinegar into a large glass of water (8–12 oz) and drink it 10–15 minutes before your two largest, most carbohydrate-dense meals of the day.
Why it works — the acetic acid mechanism:
Acetic acid, the active compound in ACV, performs two distinct biological functions simultaneously:
- Alpha-glucosidase inhibition: Acetic acid temporarily inhibits the digestive enzymes in the small intestine responsible for breaking down complex starches into glucose. This slows carbohydrate absorption and flattens the glucose curve.
- AMPK activation: Acetic acid activates Adenosine Monophosphate-Activated Protein Kinase (AMPK) — often described as the body’s metabolic master switch. When AMPK is activated, muscle cells become highly sensitized to insulin, allowing them to pull glucose out of the bloodstream with far less insulin assistance.
The research backing:
- A study published in the Journal of Functional Foods found that consuming vinegar before a high-carbohydrate meal reduced post-meal blood glucose by 20% and suppressed the subsequent insulin spike by 19%
- A separate study from Arizona State University demonstrated that consuming vinegar before bed lowered next-morning fasting blood glucose by 4% to 6%
- A 2024 meta-analysis in Nutrients pooling data from 11 randomized controlled trials confirmed that regular ACV consumption produced a statistically significant reduction in fasting insulin levels across all participant groups
Less circulating insulin means the biological lock on your chest fat is progressively dismantled with every meal.
Strategy 3: Eliminate Xenoestrogens and Ultra-Processed Foods
Controlling insulin also demands a thorough audit of the chemical composition of your diet and food storage habits. Ultra-processed foods are loaded with refined seed oils, artificial additives, and high-fructose corn syrup — all of which drive insulin resistance. But there is a less-discussed threat embedded in the packaging itself.
Xenoestrogens are industrial chemicals — most notably Bisphenol A (BPA), phthalates, and parabens — that are found in plastic food containers, canned food linings, non-stick cookware coatings, and synthetic food packaging. As detailed in a comprehensive review published in Environmental Health Perspectives, these compounds possess a molecular structure that closely mimics natural estrogen.
When ingested or absorbed through the skin, xenoestrogens:
- Bind directly to estrogen receptors in male tissue, triggering estrogenic responses
- Signal the body to deposit fat in estrogen-sensitive areas, including the chest
- Actively contribute to glandular tissue proliferation in true gynecomastia cases
- Suppress testosterone production through endocrine disruption
A 2025 study published in Environmental Research found that men in the highest quartile of urinary BPA levels had testosterone levels 17% lower than men in the lowest quartile — a staggering difference attributable entirely to chemical exposure.
Practical elimination steps:
- Switch to whole, single-ingredient foods as your dietary foundation
- Store all meals and leftovers in glass or stainless steel containers
- Never heat food in plastic containers, even those labeled “microwave-safe”
- Choose fresh or frozen vegetables over canned alternatives
- Filter your drinking water with a reverse osmosis or activated carbon filter
Strategy 4: Time-Restricted Eating for Insulin Reset
Time-restricted eating (TRE) — often called intermittent fasting — is one of the most well-researched tools for restoring insulin sensitivity. By compressing your eating window to 8–10 hours per day and fasting for 14–16 hours, you allow insulin levels to fully bottom out during the fasting period.
During this low-insulin window:
- Hormone-sensitive lipase becomes fully active, enabling genuine fat oxidation
- Growth hormone secretion surges (by up to 2,000% during extended fasts, per research in the New England Journal of Medicine), accelerating fat breakdown and muscle preservation
- Cellular autophagy — the body’s self-cleaning process — is activated, improving metabolic efficiency
A 2024 clinical trial published in Cell Metabolism found that men following a 16:8 TRE protocol for 12 weeks experienced a 34% reduction in fasting insulin and a significant reduction in visceral fat compared to controls eating the same caloric intake across a standard eating window.
Implementation approach:
- Begin your eating window at 10:00 AM or 12:00 PM
- Close your eating window by 6:00 PM or 8:00 PM
- Consume only water, black coffee, or plain green tea during the fasting window
- Maintain consistent meal timing seven days per week for hormonal rhythm
5. Pillar 2: Eliminating Androgen Suppressors and Optimizing Testosterone
Many men jump immediately to exotic testosterone-boosting supplements when they realize hormones are the issue. This is backwards. True hormonal optimization is not about adding unproven compounds — it is about aggressively eliminating the lifestyle factors that are actively suppressing your natural endocrine system. Remove the suppressors first, then optimize.
Sleep: The Ultimate Androgen Accelerator
![Split comparison visual: man with poor sleep habits vs optimized sleep showing testosterone level bars, bedroom environment tips checklist, dark blue and gold color scheme, infographic style]
The vast majority of a man’s daily testosterone is synthesized and released overnight in rhythmic pulses during slow-wave deep sleep and REM cycles. This is not a minor detail — it is the primary mechanism of testosterone production in adult men.
If you truncate your sleep, you directly truncate your testosterone output.
A landmark study from the University of Chicago restricted healthy young men to just 5 hours of sleep per night for one week. The results were alarming:
- Circulating testosterone levels crashed by 10% to 15% compared to well-rested baseline
- The researchers noted this decline was equivalent to aging 10 to 15 years in a single week from an endocrine perspective
- Cortisol levels simultaneously spiked, compounding the testosterone suppression
A 2025 analysis published in Sleep Medicine Reviews pooling data from 43 studies confirmed that every additional hour of sleep below 7 hours per night is associated with a measurable reduction in morning testosterone levels, with the effect becoming clinically significant below 6 hours.
Sleep optimization protocol:
- Maintain a strict 7.5 to 8.5-hour sleep window — consistency of timing matters as much as duration
- Cool your bedroom to 60–67°F (15–19°C); core body temperature must drop to initiate deep sleep cycles
- Eliminate all blue-light-emitting screens at least 60 minutes before bed — blue light suppresses melatonin secretion and fragments REM architecture
- Use blackout curtains or a sleep mask; even low-level ambient light disrupts melatonin and growth hormone release
- Avoid alcohol within 3 hours of sleep — while alcohol may induce drowsiness, it devastates REM sleep quality and suppresses overnight testosterone synthesis
Correcting Micronutrient Deficiencies: Zinc and Vitamin D
Without the correct raw chemical building blocks, your Leydig cells in the testes cannot physically synthesize testosterone — regardless of how well you eat or train. Two micronutrient deficiencies are overwhelmingly prevalent in modern men and directly responsible for suppressed testosterone production.
| Micronutrient | Biological Role | Target Daily Dosage | Best Sources |
|---|---|---|---|
| Zinc | Directly involved in converting cholesterol into testosterone at the cellular level; deficiency causes immediate hypogonadism | 25–40 mg Zinc Citrate or Gluconate | Oysters, red meat, pumpkin seeds, pasture-raised eggs |
| Vitamin D3 | Functions as a secosteroid hormone; binds directly to androgen receptors to stimulate testosterone synthesis | 3,000–5,000 IU daily with a fatty meal | Direct sunlight, wild-caught fatty fish, quality supplementation |
| Magnesium Glycinate | Reduces SHBG (sex hormone-binding globulin), increasing the ratio of free, bioavailable testosterone | 300–400 mg before bed | Dark leafy greens, pumpkin seeds, dark chocolate |
The research is unambiguous:
- A study published in Nutrition found that zinc-deficient men who supplemented daily for 6 months experienced a 74% increase in circulating testosterone — nearly doubling their baseline levels
- A meta-analysis in Hormone and Metabolic Research confirmed that Vitamin D supplementation significantly elevated total and free testosterone in men with baseline deficiency (below 50 nmol/L)
- A 2024 study in Biological Trace Element Research found that magnesium supplementation reduced SHBG by an average of 13% over 8 weeks, meaningfully increasing free testosterone availability
Request a comprehensive blood panel from your physician that includes total testosterone, free testosterone, SHBG, estradiol, Vitamin D (25-OH), zinc, and magnesium. Identify and correct these deficiencies before spending money on anything else.
The Cortisol Control Protocol
Cortisol is your primary stress hormone, secreted by the adrenal glands in response to psychological stress, physical overtraining, caloric restriction, and sleep deprivation. Cortisol and testosterone share an explicit, documented inverse relationship driven by a mechanism called pregnenolone steal.
Both hormones are synthesized from the same precursor molecule — pregnenolone. When your body is under chronic stress, it prioritizes cortisol production, diverting pregnenolone away from the testosterone synthesis pathway. The result is a direct, measurable reduction in testosterone output.
Research published in Hormones and Behavior found that men with chronically elevated cortisol had testosterone levels up to 20% lower than their relaxed counterparts. More critically, cortisol directly increases aromatase expression within fat tissue — meaning high stress simultaneously robs you of testosterone and accelerates its conversion into chest-fat-building estrogen.
Practical cortisol reduction strategies:
Omega-3 Fatty Acids:
Integrate wild-caught fatty fish (salmon, mackerel, sardines, herring) into your diet 3–4 times per week. A study from the University of Gettysburg found that supplementing with 4 grams of fish oil daily reduced baseline cortisol levels by 19% over 6 weeks while simultaneously reducing body fat percentage. If dietary fish intake is inconsistent, supplement with a high-quality triglyceride-form omega-3 providing at least 2–3 grams of combined EPA and DHA daily.
Ashwagandha (KSM-66 extract):
A double-blind, placebo-controlled trial published in the Journal of the International Society of Sports Nutrition found that men taking 600 mg of KSM-66 ashwagandha daily for 8 weeks experienced a 27.9% reduction in cortisol and a 15.4% increase in testosterone compared to placebo. This is one of the most well-replicated findings in adaptogen research.
Zone 2 Cardio (not HIIT):
Contrary to popular belief, high-intensity interval training performed excessively actually elevates cortisol significantly. Moderate-intensity Zone 2 cardio — maintaining 60–70% of maximum heart rate for 30–45 minutes — has been shown to reduce cortisol and improve hypothalamic-pituitary-adrenal (HPA) axis regulation without the cortisol spike associated with maximal-effort exercise.
Avoid the Crash Diet Trap
When men want to eliminate chest fat quickly, the instinct is to slash calories aggressively. This is one of the most common and damaging biological errors in male fat loss.
Research published in the Journal of Clinical Endocrinology revealed that severe caloric restriction — defined as eating more than 40% below maintenance calories — produces the following within just 14 days:
- Cortisol spikes by up to 35% system-wide
- Testosterone plummets by up to 36%
- Muscle protein synthesis decreases significantly, accelerating lean mass loss
- Metabolic rate adapts downward through reduced thyroid hormone output
A crashed endocrine system does not burn chest fat — it protects it while consuming muscle tissue. The hormonal environment created by crash dieting is nearly identical to the hormonal environment that causes chest fat accumulation in the first place.
The correct approach:
Maintain a moderate, sustainable caloric deficit of 300 to 500 calories below your Total Daily Energy Expenditure (TDEE). This is the evidence-based sweet spot that:
- Preserves testosterone and anabolic hormone output
- Protects lean muscle mass
- Forces consistent fat oxidation without triggering starvation adaptations
- Is sustainable for the 16–24 weeks required to produce meaningful changes in stubborn fat deposits
Calculate your TDEE using the Mifflin-St Jeor equation adjusted for your activity level, then subtract 300–500 calories. Recalculate every 4 weeks as your body weight changes.
6. Pillar 3: Fasted Training Protocols and Optimizing the Fat-Burning Window
To accelerate chest fat removal, you must capitalize on the periods when insulin is at its absolute lowest and fat oxidation is at its physiological peak. This requires understanding how to strategically time your training and structure your exercise selection.
The Fasted Morning Training Window
During the overnight fast, insulin levels reach their daily nadir. Growth hormone — which directly stimulates lipolysis and fat oxidation — peaks during the final hours of sleep and remains elevated in the early morning hours. This creates a narrow but powerful window for accelerated fat burning.
Fasted cardio protocol for chest fat:
- Train within 30–60 minutes of waking, before consuming any calories
- Consume black coffee or green tea 20 minutes before training — both compounds (caffeine and EGCG) have been shown to further elevate catecholamines and enhance fat oxidation during exercise
- Perform 30–45 minutes of Zone 2 cardio (brisk walking on an incline, cycling, rowing) at 60–70% maximum heart rate
- A 2024 study in the International Journal of Sport Nutrition and Exercise Metabolism confirmed that fasted Zone 2 cardio oxidized 20–30% more fat per session compared to the same workout performed in a fed state
Resistance Training: Compound Movements Over Isolation
Here is the counterintuitive truth about chest training for fat loss: heavy compound movements that recruit the most total muscle mass are dramatically more effective than chest isolation exercises for eliminating chest fat.
The reason is hormonal. Heavy compound lifts — squats, deadlifts, barbell rows, overhead presses — trigger a significant acute spike in testosterone and growth hormone that persists for 15–30 minutes post-exercise. This hormonal surge creates a systemic fat-oxidizing environment that affects the entire body, including estrogen-dominant fat deposits on the chest.
Chest isolation exercises like cable flyes and pec deck machines produce a fraction of this hormonal response because they recruit far less total muscle mass.
Optimal resistance training structure for chest fat elimination:
| Training Variable | Recommendation | Rationale |
|---|---|---|
| Primary movements | Squat, deadlift, barbell row, overhead press | Maximum hormonal response per session |
| Secondary movements | Incline press, dips, push-up variations | Chest development and posture improvement |
| Rep range | 4–8 reps for compound, 8–12 for accessory | Maximizes testosterone response |
| Rest periods | 2–3 minutes between heavy sets | Allows full hormonal recovery |
| Training frequency | 4 days per week | Sufficient stimulus without cortisol overload |
| Session duration | 45–60 minutes maximum | Beyond 60 minutes, cortisol rises significantly |
The Posture Factor: Why It Matters More Than You Think
One frequently overlooked contributor to the appearance of chest fat is anterior pelvic tilt and kyphotic posture — a forward-rounded shoulder position that causes the chest to droop and the pectoral region to appear softer and fuller than it actually is.
Strengthening the posterior chain (rear deltoids, rhomboids, mid-trapezius, thoracic extensors) and stretching the anterior chest and hip flexors can dramatically improve chest appearance — sometimes making a visible difference within weeks, even before significant fat loss occurs.
Include in every training week:
- Face pulls: 3 sets × 15–20 reps
- Band pull-aparts: 3 sets × 20 reps
- Thoracic extension over a foam roller: 2 minutes daily
- Doorway chest stretches: 3 × 30-second holds
7. The Complete Weekly Protocol: Putting It All Together

Understanding the biology is one thing. Executing a coherent, weekly system is what produces results. Here is a complete, integrated protocol designed to address every hormonal and metabolic driver of chest fat simultaneously.
Daily Non-Negotiables
- Wake up → Drink 16 oz of filtered water before anything else
- Pre-breakfast → ACV protocol (1 tbsp in 8 oz water) if eating breakfast; skip if fasting
- Every meal → Follow protein → fiber → carbohydrate sequencing strictly
- Eating window → 10 AM to 6 PM (or 12 PM to 8 PM) — choose one and maintain it consistently
- Evening → No screens 60 minutes before bed; bedroom cooled to 65°F
- Sleep → 7.5–8.5 hours, consistent wake time seven days per week
Weekly Training Structure
| Day | Training Focus | Duration |
|---|---|---|
| Monday | Heavy lower body (squat focus) + 20 min fasted Zone 2 | 60 min |
| Tuesday | Fasted Zone 2 cardio only | 40 min |
| Wednesday | Upper body push/pull (compound focus) + posture work | 55 min |
| Thursday | Active recovery (walking, mobility, stretching) | 30 min |
| Friday | Heavy lower body (deadlift focus) | 55 min |
| Saturday | Upper body + chest accessory work + posture | 55 min |
| Sunday | Complete rest or light walking | — |
Supplement Stack (Evidence-Based Only)
| Supplement | Dose | Timing | Purpose |
|---|---|---|---|
| Zinc Citrate | 30 mg | With dinner | Testosterone synthesis support |
| Vitamin D3 + K2 | 4,000 IU D3 / 100 mcg K2 | With largest meal | Androgen receptor activation |
| Magnesium Glycinate | 400 mg | 30 min before bed | SHBG reduction, sleep quality |
| KSM-66 Ashwagandha | 600 mg | Morning or evening | Cortisol reduction, testosterone support |
| Omega-3 (EPA+DHA) | 3 g combined | With a meal | Cortisol reduction, aromatase modulation |
| Creatine Monohydrate | 5 g | Post-workout | Lean mass preservation, DHT support |
8. Timeline: What to Realistically Expect
One of the most damaging mistakes men make when learning how to get rid of chest fat is expecting rapid, linear results. Hormonal rebalancing is a biological process — it operates on its own timeline, and that timeline must be respected.
Weeks 1–4: The Foundation Phase
- Insulin sensitivity begins improving within the first 7–10 days of implementing food sequencing and TRE
- Sleep optimization produces measurable improvements in morning testosterone within 2 weeks
- Zinc and Vitamin D supplementation requires 4–6 weeks to meaningfully elevate serum levels
- Scale weight may not change dramatically, but energy levels, libido, and morning erections (reliable proxies for testosterone status) typically improve
Weeks 5–12: The Momentum Phase
- Aromatase activity begins declining as visceral fat decreases
- Testosterone-to-estrogen ratio improves measurably — a repeat blood panel at week 8 should show progress
- Chest fat begins responding to caloric deficit; the hormonal environment is no longer actively fighting against fat loss
- Visible changes in chest shape become apparent, particularly reduction in nipple puffiness
Weeks 13–24: The Transformation Phase
- Sustained hormonal optimization produces compounding benefits — lower aromatase, higher testosterone, improved insulin sensitivity reinforce each other
- Chest fat continues to respond proportionally to overall body fat reduction
- Men who began with mild-to-moderate hormonal gynecomastia often see significant improvement in nipple appearance and chest contour
- Body fat percentage typically drops 4–8% over this period when the full protocol is consistently applied
Important: If you implement this protocol consistently for 16+ weeks and see no measurable improvement in hormonal markers or chest appearance, consult an endocrinologist. Some cases of true gynecomastia — particularly those involving established glandular tissue — may require medical intervention including selective estrogen receptor modulators (SERMs) or, in persistent cases, surgical consultation.
Conclusion: The Biological Path Forward
Stubborn chest fat is not a willpower problem. It is not a workout intensity problem. It is a hormonal environment problem — and it demands a hormonal environment solution.
The aromatase vicious cycle, chronic hyperinsulinemia, cortisol-driven testosterone suppression, and xenoestrogen exposure are the real architects of male chest fat. Chest presses and crash diets do not address any of these mechanisms. They treat the symptom while the cause continues operating unchecked.
The protocol outlined in this guide — insulin re-engineering through food sequencing and time-restricted eating, testosterone optimization through sleep and micronutrient correction, cortisol management through omega-3s and adaptogens, and strategic fasted training — attacks the problem at every biological level simultaneously.
This is not a quick fix. Hormonal rebalancing takes weeks and months, not days. But the results it produces are permanent — because you are changing the underlying biochemical environment, not just temporarily masking the symptom.
Commit to the system. Trust the biology. The chest you want is not out of reach — it is on the other side of understanding what has actually been holding you back.
Always consult a qualified physician or endocrinologist before beginning any supplementation protocol or making significant dietary changes, particularly if you suspect true hormonal gynecomastia or have pre-existing medical conditions.